Hipaa Authorization Form Kentucky
Caccessintelligent Formcommonprojectuoflhealth2c2018 Eps
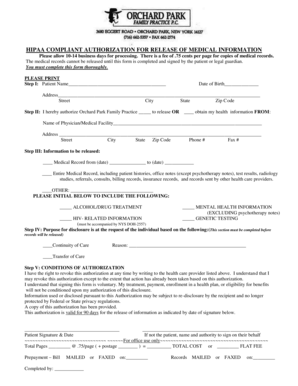
• i understand that i have a right to a copy of this authorization, and that a photocopy or facsimile is as valid as the original. hipaa authorization form kentucky • california residents are entitled to a large print version of this form by calling (800) 541-2254 to request form healthmedauth-large. 8. Patient authorization for release of medical information this form allows lsi, llc to send records on your behalf laser spine institute, llc medical records department 3031 n. rocky point drive, e. tampa, fl 33607 phone: 813-289-9613 fax:. Hippa release forms allow you to provide others access to your protected medical records, most often to other doctors or care providers. however, this form can also be used to release your medical information to a specific person. use the hipaa authorization form document if:. Hipaa guidance for requesting and completing waiver of authorization (revised 6/4/04) what is hipaa? the health insurance portability and accountability act (hipaa) is a complex regulation that affects many researchers at the university of kentucky.

Free Hipaa Authorization Form Free To Print Save Download
4. this authorization expires: date: _____ this authorization is subject to written revocation at any time except to the extent that the health care provider has already taken action in reliance on the authorization. **as of march 22, 2021, we will begin to vaccinate first doses for phase 1a, and phase 1b, tiers 1 and 2. this includes, but not limited to, healthcare workers, first responders, teachers/childcare providers, 65+ years old, and 16-64 years old with pre-existing condtions. Sample hipaa right of access form for family member/friend providers and payers to disclose and release my protected health information described.
Moderna: covid vaccine consent form (federal partner) * prior to filling this form out you will need photos of your social security card and medicare part b (red, white and blue card). if you are commercially insured you will need to provide your pharmacy benefits insurance card. For example, an authorization may expire "one year from the date the authorization is signed," "upon the minor’s age of majority," or "upon termination of enrollment in the health plan. " an authorization remains valid until its expiration date or event, unless effectively revoked in writing by the individual before that date or event. Documents incorporated by reference the information required by part iii of this annual report on form 10-k, to the extent not set forth in this form 10-k, is incorporated herein by reference from. The kentucky employees’ health plan (“kehp”) collects and maintains protected health information (“phi”) (“hipaa”), kehp and its business associates may use and disclose your phi for treatment, payment, or health care operations this authorization is voluntary and you may refuse to sign it.
Authorization (unless treatment is sought only to create health information for a third party or to take part in a research study) and that i may have the right to refuse to sign this authorization. i will receive a copy of this authorization after i have signed it. a copy of this authorization is as valid as the original. Louisville, ky 40204. 855-852-7005. hipaa authorization form. this form lets humana i caresource® share your protected health information. (phi) as . Showing information for kentucky type size. typesize hipaa resource center pharmacy prior hipaa authorization form kentucky authorization request form; prior authorization pre-service review guide & request form (please use this form to request a pa for medically billed drugs (jcode).
Dob______________, hereby authorize the above facility to protected by federal privacy law (also known as hipaa) and that the recipient of my health information management, attn: release of information, p. o. box 3407, louisville,. University of kentucky a. b. chandler hospital uk healthcare good samaritan hospital uk healthcare ambulatory services uk dental and oral health clinics l l l l page 1 of 2 authorization for release of information (for use and disclosure) please fill out all sections or the form may be returned to you. patient name: social security number:. What is a hipaa authorization form? hippa release forms allow you to provide others access to your protected medical records, most often to other doctors or .
Hipaa authorization for disclosure of personal.
Model authorization form under hipaa* this form should be used when release of a patient’s protected health information is being made to anyone for a purpose other than treatment, payment or health care operations. the form should be adapted to meet the needs of a particular situation and a particular physician practice. releases in which. The hipaa law to protect patient health information is quite well known by personnel in most physician offices. there still remain, hipaa authorization form kentucky however, some questions regarding hipaa's rules and regulations.
authorization has been obtained in advance in the form of a return material authorization (“rma”) number, and the items are received by authorization has been obtained in advance in the form of a return material authorization (“rma”) number, and the items are received by Hipaa privacy authorization form. **authorization for use or disclosure of protected health information. (required by the health insurance portability and .
Form 106 adopted july 2003 this authorization shall remain valid for 180 days following its execution. a photocopy of the authorization may be accepted in lieu kentucky workers’ compensation and hipaa on april 14, 2003, the federal health insurance portability and accountability act [hipaa] privacy regulation will take effect. Oca official form no. : 960 authorization for release of health information pursuant to hipaa [this form has been approved by the new york state department of health] patient name date of birth social security number patient address i, or my authorized representative, request that health information regarding my care and treatment be released as.
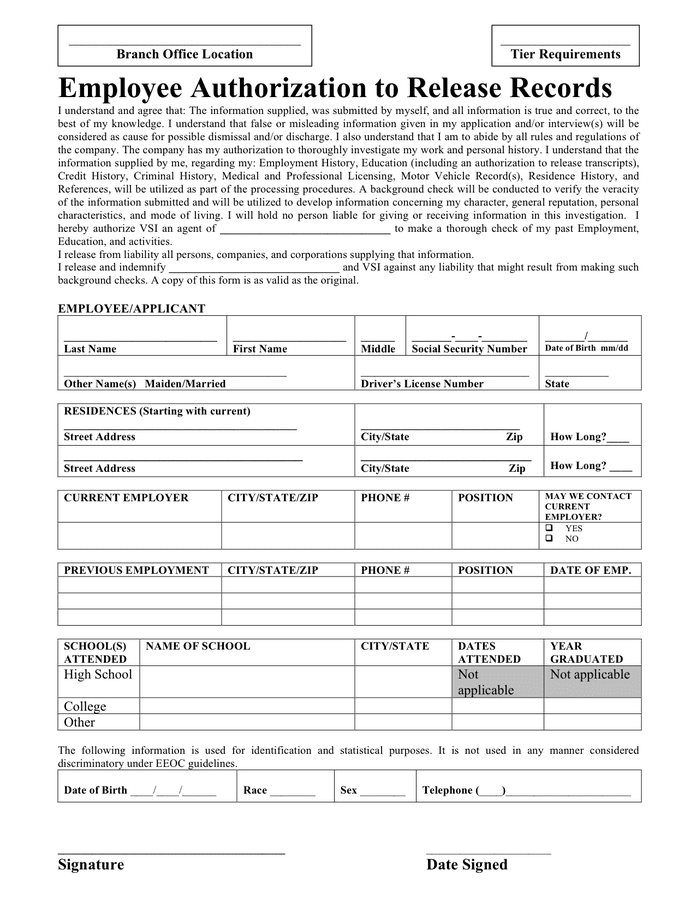
A hipaa authorization to disclose protected health information, also known as a hipaa release, is a legal document providing healthcare workers with the ability to disclose a patient's private medical information to other specified third-parties. Model authorization form under hipaa*. this form should be used when release of a patient's protected health information is being made to anyone for a . Kentucky. hipaa authorization (patient) (ky) this form creates a hipaa authorization form, which enables certain trusted family and friends to have access to your medical records and health information when you are injured. these records are typically used to help prove whether you are capable to make health care and financial decisions on your. The medical record information release (hipaa), also known as the ‘health insurance portability and accountability act’, is included in each person’s medical file. this document allows a patient to list the names of family members, friends, clergy, health care providers, or other third (3rd) parties to whom they wish to have made their medical information available.
Hipaa release form author: caring. com subject: free hipaa release form keywords: hipaa release form, free hipaa release hipaa authorization form kentucky form, hipaa form, hippa form, free hipaa form, free hippa form, hipaa medical form, hipaa consent form, hipaa compliance form, hipaa medical release form created date: 20090918203958z. Pursuant to the health insurance portability and accountability act (hipaa) privacy regulations, 45 cfr i hereby authorize a free copy of my medical records pursuant to krs 422. 317 be sent, to the extent i have state of kentucky. I understand the benefits and risks of the covid-19 vaccine as described in the emergency use authorization (eua), a copy of which i was provided with this consent and release. i have had a chance to ask questions that were answered to my satisfaction.


{kind=link}
Post a Comment for "Hipaa Authorization Form Kentucky"